Istanbul · Male Chest Surgery
Discreet, gynecomastia surgery.
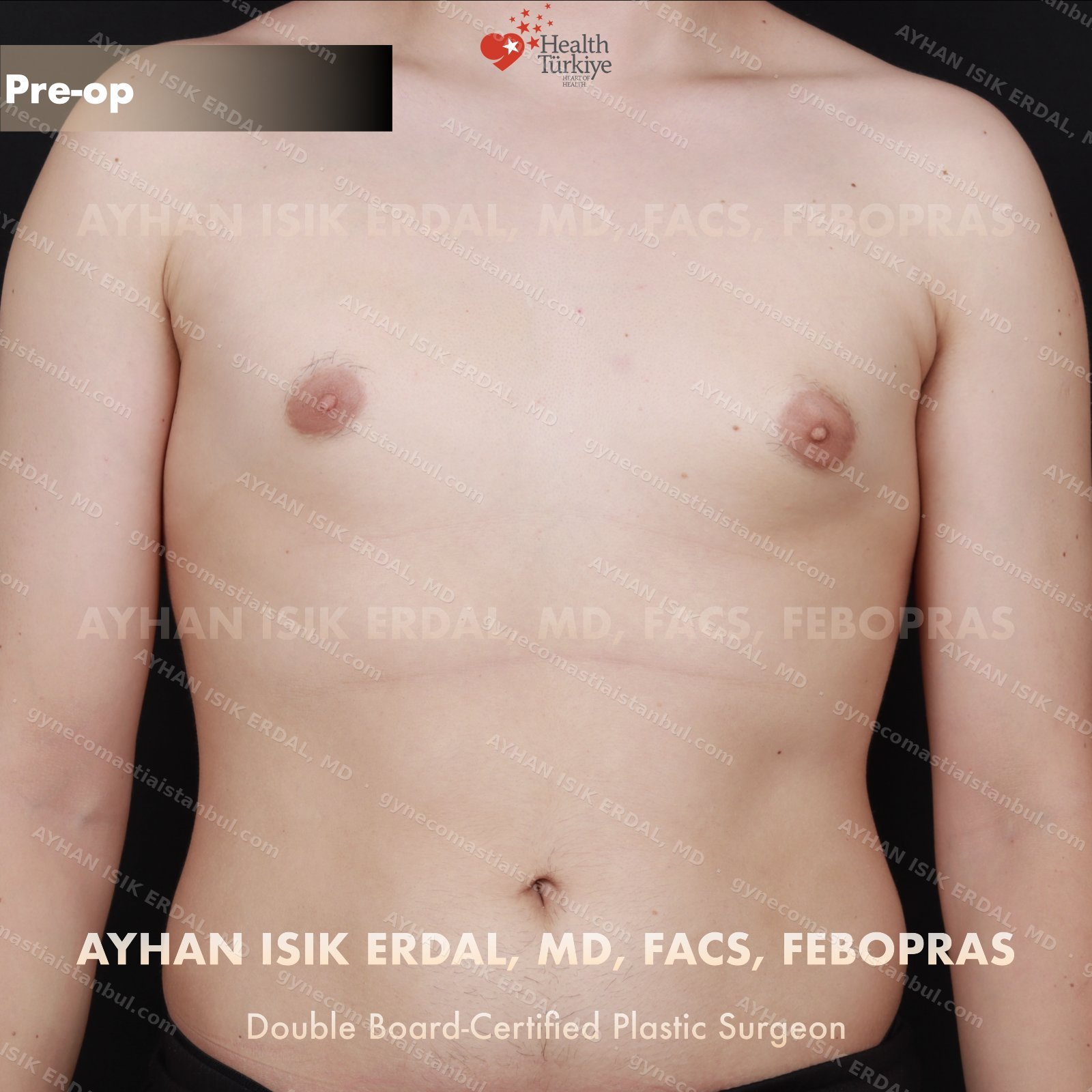
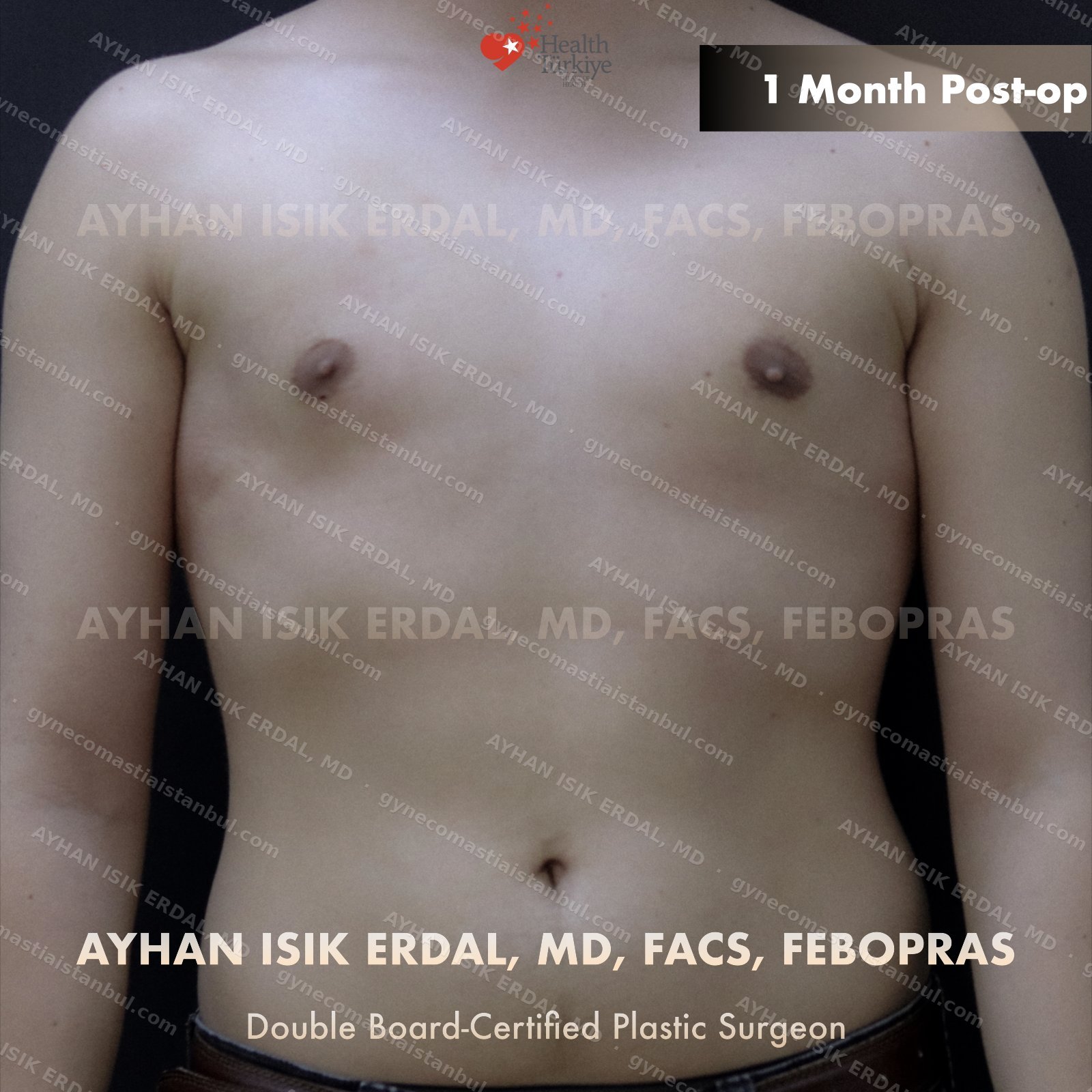
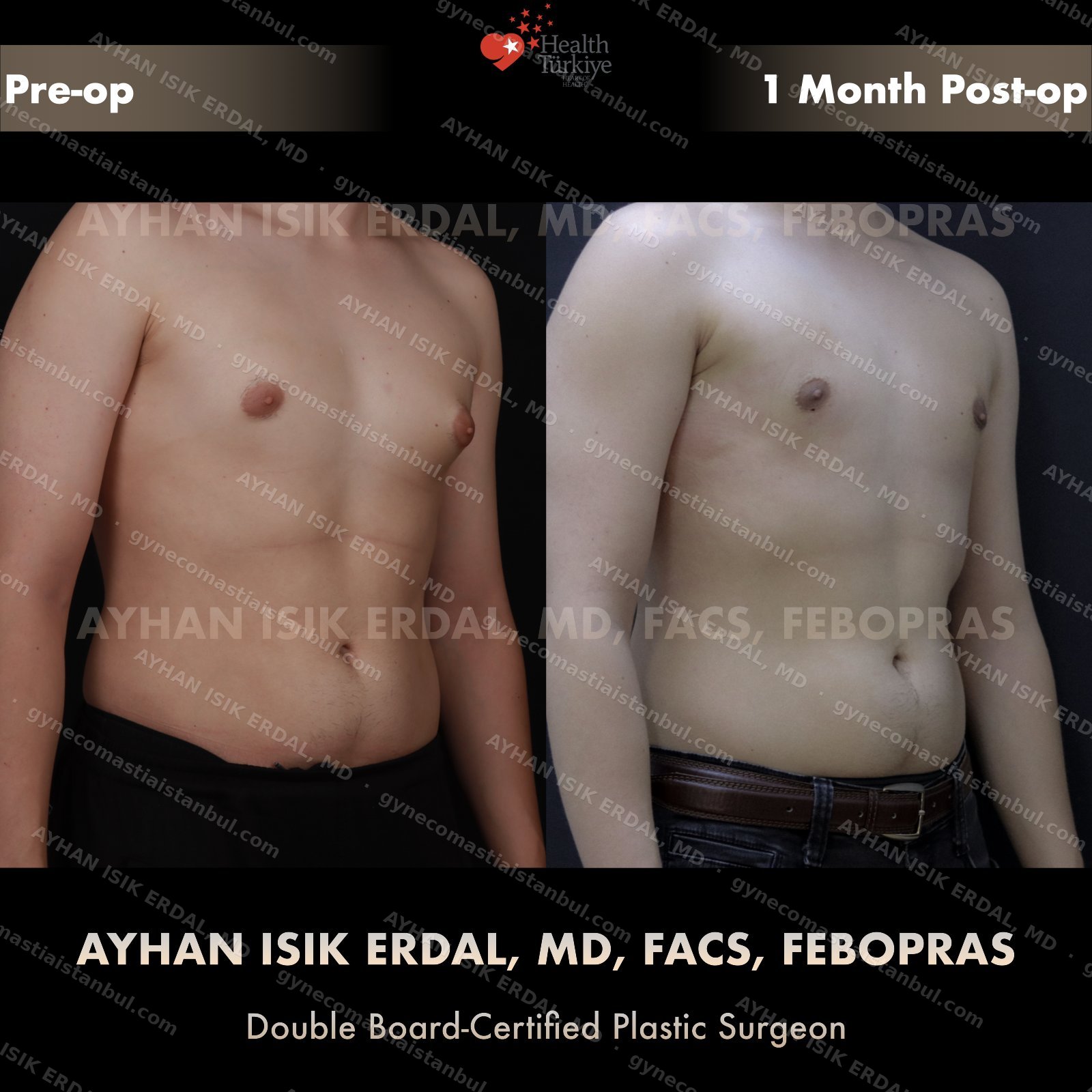
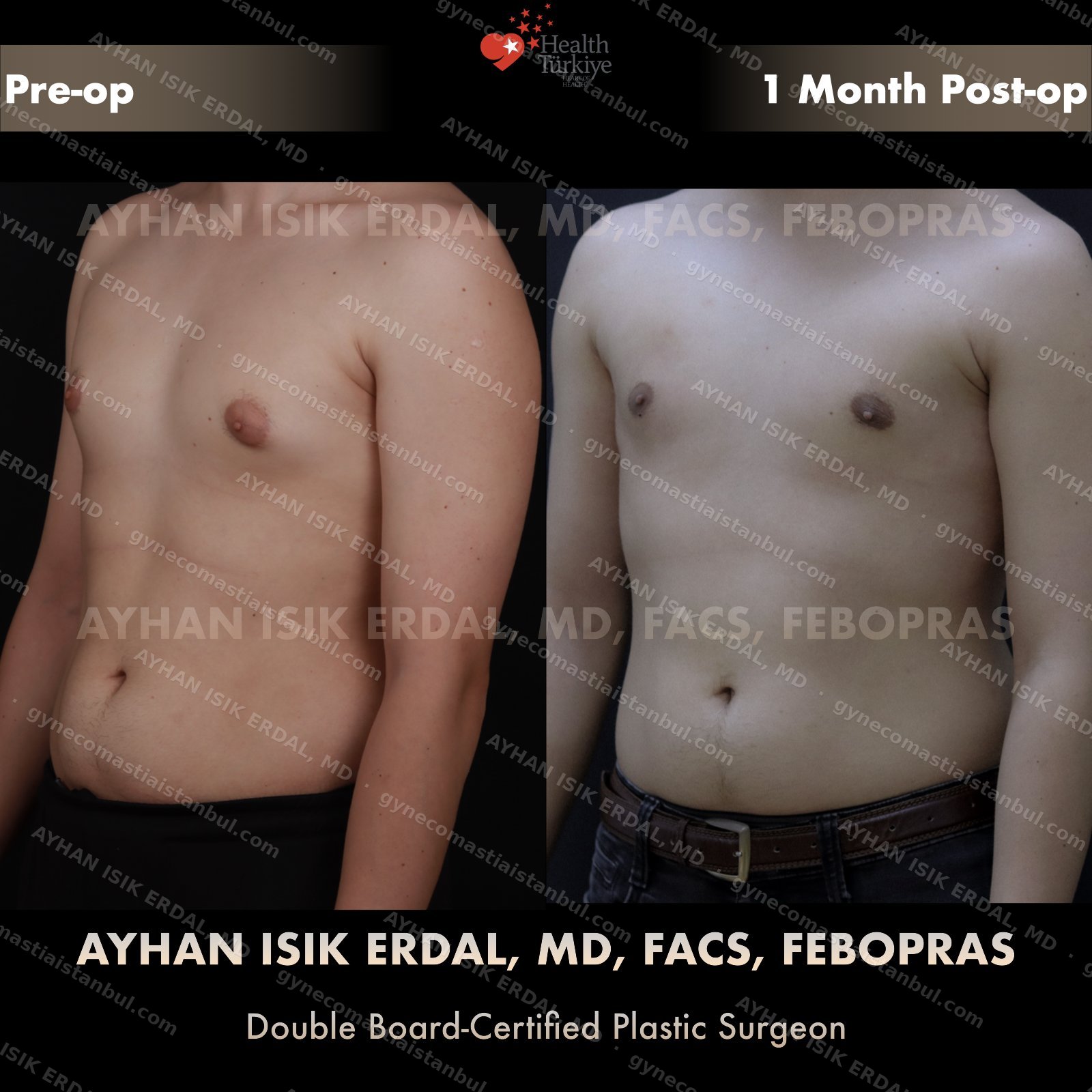
Gynecomastia is common. Talking about it is harder than it should be. Assoc. Prof. Dr. Ayhan Işık Erdal offers a confidential, judgement-free consultation — and a surgical plan matched to your Simon grade, not to a one-size-fits-all protocol. Periareolar scar hides at the natural areolar border. Liposuction, pull-through or gland excision, selected by anatomy.
F
FACS
American College of Surgeons
E
FEBOPRAS
European Board of Plastic Surgery
30+
Peer-reviewed publications
ASJ, PRS, Annals of Plastic Surgery
A+
Accredited hospitals
MoH international authorization

Fellow · FACS
American College of Surgeons · 2025